99mTc-Sestamibi (MIBI) is an increasingly used tool for evaluation of thyroid nodules.The utility of MIBI for the differentiation of thyroid nodules in a large cohort. In one of the European study 161 patients underwent MIBI, followed by a thyroidectomy. We used a dual phase MIBI protocol. Interpretation of the images included a scoring system from 0 (absent) to 3 (increased); this was to provide a scale for the uptake of the thyroid nodule in comparison to the paranodular tissue. Additionally, evaluated the tracer uptake trend in late images compared to early images and also used final histopathology as the reference standard. Scores 0-1 in early images, scores 0-2 in late images, and an absence of increasing uptake in the thyroid nodule in late images, showed the best predictive values to exclude malignancy, respectively (negative predictive value (NPV) 89%). Highest sensitivity (91%) for malignant nodules was evident in early images with a score 1-3. Highest specificity (91%) was obtained when the negative was defined as an absence of uptake-increase, in the late images. This study confirms that the most valuable feature of MIBI is the high NPV. Thus, with the appropriate interpretation method, high sensitivity and specificity, and moderate PPV can be obtained.
29 years old male with history past renal transplant, high PTH ( 253 ng/ml) and hypercalcemia.10.3 mg/dl refered for sestamibi parathyroid scintigraphy for the further work up.
Biochemical parmeters- serum creatinine 1.5 mg/dl, glucose 113mg/dl and serum potassium 4.6 mmol/L
Bilateral superior parathyroid glands are not visulised, inferior right parathyroid appears normal in size and shows hyper echoic echotexture measuring 9.4*3.8 mm ? adenoma. Lobulated heterogenous lesion with cystic areas and mild vascularity nad peripheral calcification is seen in left lobe measuring 21*10 mm.
Early and Delayed mibi images of neck and chest It shows area of increased MIBI tracer uptakes in upper 2/3rd portion of left lobe on early images (as apprciated in static and SPECT-CT fused images) and adequate washout pattern seen on delayed images. No focal area of any abnormal tracer uptakes seen in mediastinal region
The right lobe measures 4.2*1.8 cms in size and left lobe 3.5*1.9 cms in size approximately. Upper 2/3rd of left lobe shows comparatively decreased tracer uptakes, while rest of the gland shows good but mildly patchy tracer uptakes
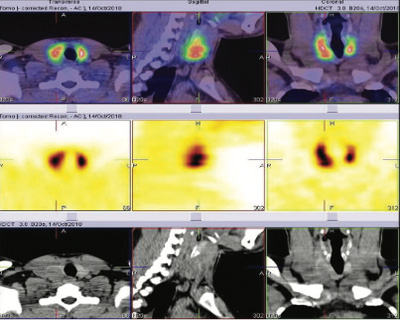
SPECT-CT FUSED images shows-1.4*1.1 cms approximate sized nodule in left lobe posteriorly ( on CT IMAGES ), While SPECT images it appears to be cold, while surrounding area shows more tracer uptakes.
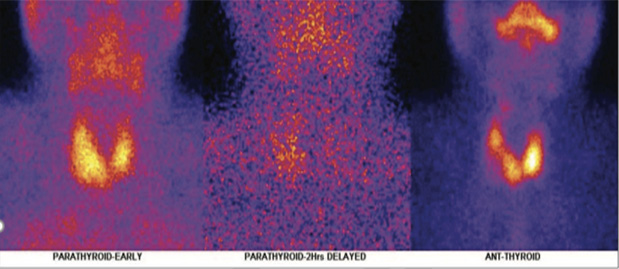
It has been reported as 99mTC- THYROID SCAN-There is cold nodule in left lobe of thyroid gland posteriorly (appreciated in spect- ct fused images) and warm nodule pattern on static images ( because of overlying activity).
99mTc- SESTAMIBI SCAN- The upper 2/3rd portion of left lobe shows increased mibi tracer uptakes on initial images and adequate washout paettern on delayed images and it is matching with tc thyroid static and spect-ct fused images of left lobe.
in view of above findings, it looks more likely to be metabolically active thyroid nodule in left lobe posteriorly and less likely to be left lobe intra-thyoridal parathryoid adenoma.
Cytology of the left lobe nodule- features suggestive of papillary carcinoma.
Subsequently patient underwent total thyroidectomy and histopathology showed multifocal differential conventional papillary carcinoma of thyroid involving left lobe, isthumus, right lobe with metastasis to three out of three central compartment nodes with perinodal extension.
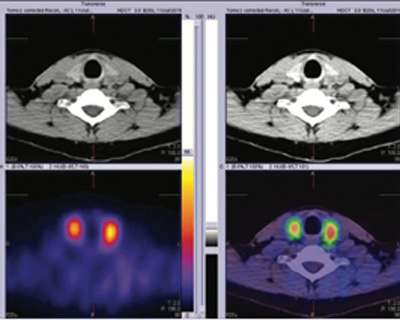
Parathyroid early SPECT-CT fused images 1 shows increased MIBI tracer accumulation in upper 2/3rd portion of left lobe

Thyroid SPEC-CT fused images 2 shows cold nodule in the left lobe of thyroid gland posteriorly.
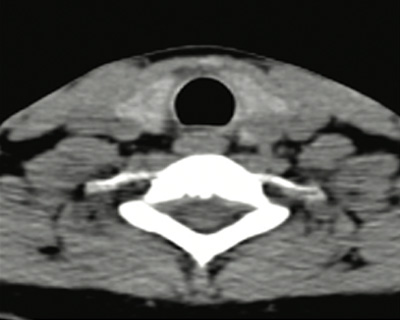
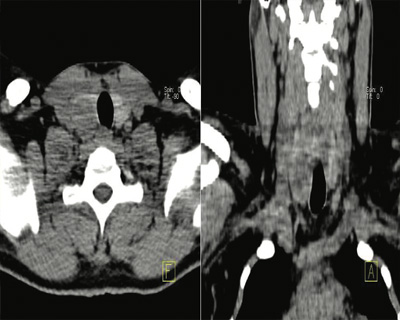
Corresponding CT images 3 shows well defined nodule in the left lobe of thyroid gland posteriorly.
28 years old male with history high PTH ( 70.2 pg/ml) and hypercalcemia.(2.80 mmol/L) refered for 99mTc-Sestamibi parathyroid scintigraphy for the further work up.
Biochemical parmeters- TSH 0.485 microIU/mL (0.35-4.94), FT4 15.4 pmol/L serum creatinine 1.5 mg/dl, glucose 113mg/dl and serum potassium 4.6 mmol/L
Right lobe shows a huge single oval circumscribed mass lesion with intra-lesional cyst, it is vascular by Doppler and elastography confirmed its nature soft ( measures 2.5*2.5Z*3.4 cm (TI-RADS 3)
Large cold nodule seen in right lobe on Tc thyroid scan shows increased MIBI tracer uptakes on initial images and minimal tracer retention on delayed images.
Rest of the thyroid gland shows good MIBI tracer uptakes on initial images and adequate washout pattern on delayed images.
No obvious focal area abnormal MIBI tracer uptake seen in thyroidal bed nor in mediastinum (Even not appreciated in SPECT-CT fused images)
The right lobe measures 5.4*3.7 cms in size and left lobe 4.0*2.3 cms in size approximately. Large cold area is seen in inferio-lateral portion of the right lobe. Areas of reduced tracer uptakes seen in upper portion of both the lobes. Rest of the gland shows mildly patchy tracer uptakes.
Present study is negative for metabolically active parathyroid abnormality (adenoma). Large sized metabolically active thyroid nodule is seen in inferio-lateral portion of the right lobe. Underwent right lobe of thyroid and parathyroid, hemithyroidectomy and excion of parathyroid
Histopathology Minimally invasive follicular carcinoma ( 3.5 cms tumor), chronic lymphocytic thyroiditis, parathyroid gland unremarkable in appeareance.
Revison surgery of the remainining thyroid gland (left lobe and isthumus) Histopatholgy shows nodular adenomatous hyperplasia with no eveidence of neoplasia.
99mTc-SESTAMIBI could be helpful in preoperative assessment of thyroid nodules. Intense MIBI activity increases the probability of thyroid cancer, whereas reduced activity drastically decreases the probability of malignancy (2001 john wiley & sons, Inc. Head and neck 23:305-310,2001.
It can also be useful with non diagnostic cytology (A negative MIBI scan in a cold nodule accurately excludes malignancy when US-FNAC is reported as non diagnostic. This avoids for more invasive diagnostic procedures. MIBI scoring system were considered positive if there was uptake superior to normal thyroid tissue on early and delayed images-score =3 ( Luca Giovanella, Sergio suriano et all, PMID 19693945 and DOI 10.1002/hed.21229).
Parathyroid images 1 & 2 shows increased MIBI tracer accumulation in inferiolateral portion of right lobe on early images and mild persistent MIBI retention on delayed images. Thyroid image 3 shows large cold area in inferio-lateral portion of the right lobe.
Parathyroid early SPEC-CT fused images 4 shows increased MIBI tracer accumulation in inferio-lateral portion of right lobe
Corresponding CT images 5 & 6 shows well defined nodule in inferio-lateral portion of right lobe