This is the most common functioning islet cell tumour. It arises from the beta cells of the pancreas and produces hypoglycaemia due to insulin secretion. Mostly insulinomas behave in a benign manner (90%) and they are generally solitary (usually less than 2 cm in size). About 5% are associated with MEA I and in these situations, there may be multiple lesions.
61 years old male with history of recurrent episodes of hypoglycaemia.
Ref for WHOLE BODY & SPECT CT OCTREOSCAN with suspected insulinoma for the diagnostic work up and look for any spread of the disease process.
99mTc-Tektrotyd Octreoscan- It showed isolated (somatostatin receptor expression (SRS) Lesion/tumour in MID portion of the body of the pancreas (better appreciated on SPECT-CT fused images as shown in picture). Rest of the whole-body images were unremarkable.
After complete work, patient underwent surgical removal of insulinoma (Neuro endocrine tumour of pancreas).
Subsequently found to have high calcium and high PTH (hyperparathyroidism) and referred for 99mTc-SESTAMIBI parathyroid scan
99mTc-SESTAMIBI scan shows fairly large sized parathyroid adenoma, inferio-lateral to left lobe of thyroid gland) as shown in pictures).
Operated and removed Parathyroid adenoma with Re-implantation of parathyroid gland in left biceps area.
Somatostatin receptors have been demonstrated in endocrine cells throughout the body, as well as in numerous endocrine tumors. Somatostatin shown to inhibit excessive production of hormones, including caused by variety of neuroendocrine tumors, including carcinoids, VIPoma’s, gastronome and insulinomas. In addition, research has shown that radiolabeled forms of somatostatin analogues bind to somatostatin receptors on tumors, allowing sensitive visualization of primary neuroendocrine tumors and their metastases.
The main indications for Octreotide scintigraphy is the imaging of Neuroendocrine tumors (such as GEP), which usually displays high density of somatostatin receptors.
In the management of patients with Neuroendocrine tumors
a) Localize primary tumors and detect sites of metastatic disease (staging and restaging).
b) Detect relapse or progression of disease (F.U of patients with known disease).
c) Monitor effects of surgery, radiotherapy or chemotherapy.
d) Predict the response of therapy as prognostic parameter.
e) Select the patients for radionuclide therapy.
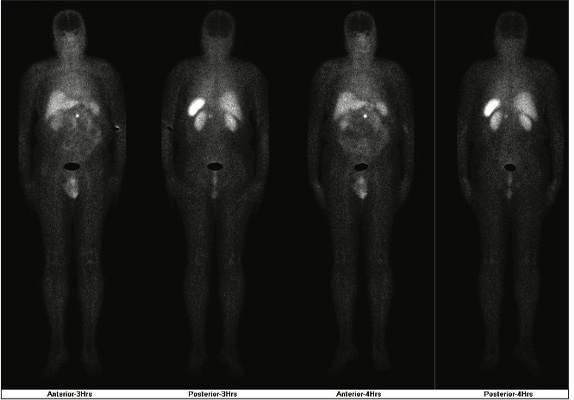
99mTc-Tektrotyd Octreo scan (WB)
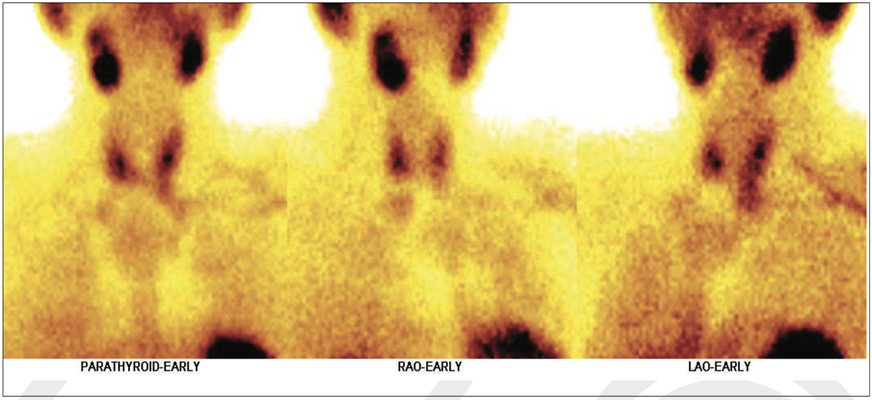
99mTc-SESTAMIBI scan shows fairly large sized parathyroid adenoma, inferio-lateral to left lobe of thyroid gland.
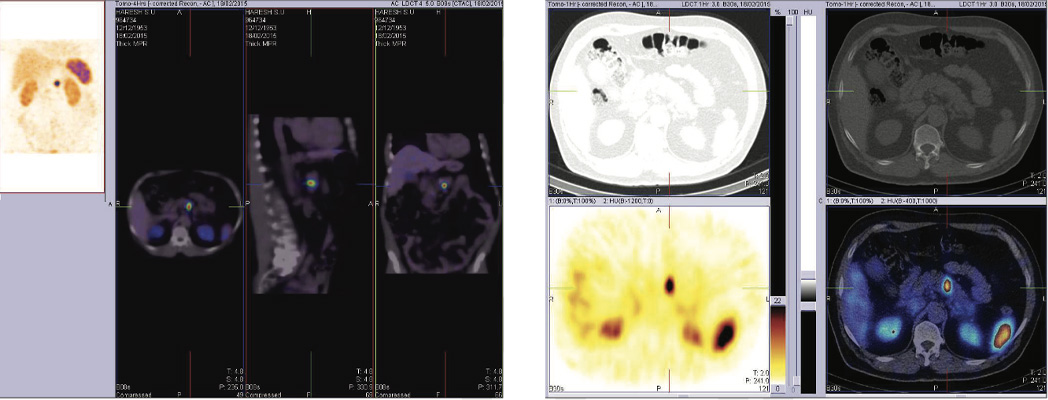
SPECT-CT IMAGES shows isolated (somatostatin receptor expression (SRS) Lesion / tumour in MID portion of the body of the pancreas (better appreciated on SPECT-CT fused images). Rest of the whole body images were unremarkable.