Degenerative facet joints are a recognized cause of persistent chronic spinal pain. Facet joint arthropathy has been identified as a source of pain in 15– 45 % of patients with chronic low back pain lasting over six weeks that have failed conservative management and in 39 % of patients with chronic cervical pain. Spinal facets can cause localized spinal pain as well as referred dermatomal pain to the head, chest wall, upper and lower extremities. Establishing a clear diagnosis of LBP is essential to providing appropriate treatment early and improving outcomes. However, the association between abnormal findings on traditional imaging techniques (plain radiography, computed tomography (CT), and magnetic resonance (MR)), clinical symptoms, and exact structure(s) involved is not straightforward, with multiple factors likely to be implicated to different degrees. Moreover, in many elderly individuals, the diagnosis of degenerative spinal disease is a non-specific finding of LBP, as degenerative changes are commonly identified in asymptomatic individuals. The causes of lower back pain are wide ranging and can be broadly divided into musculoskeletal and systemic causes.
Musculoskeletal causes
Bone: Fracture, Spondylosis, Spondylolisthesis
Joints: Facet joint disease
Disc: Hermiation, Annular tears
Ligaments: Hypertrophy, OssificationMuscular
Systemic causes
Infection: Osteomyelitis, Spondylodiscitis, Epidural abscess
Inflammation: Rheumatiod arthritis, Ankylosing spondylitis
Neoplastic: Primary tumors, Metastatic cancer, Lymphoma, Multiple myeloma Reffered pain
Magnetic resonance imaging (MRI) has been the gold standard for spinal imaging. However, diagnosis of facet joint arthropathy continues to pose a challenge to clinicians. Conventional radiological techniques such as MRI, plain computed tomography (CT), dynamic bending films and planar radionuclide bone scanning are inconsistently reliable when diagnosing or accurately localizing faceto-genic pain generators.
Radionuclide bone scintigraphy with single photon emission computed tomography (SPECT) provides functional imaging and is used to detect microcalcification due to increased osteoblastic activity. In the absence of other pathology, the foci of increased osteoblastic activity reflect areas of mechanical stress and degenerative change in the skeleton. Development of multimodality SPECT/CT has allowed the high sensitivity of SPECT to be combined with the specificity of CT allows assessment of both morphology and physiology in a single study. CT images provide a precise anatomical localization of the site (s) of radiotracer uptake, despite spinal degenerative changes, which improves the accuracy and specificity of the diagnosis of LBP. CT images also provide additional structural detail about anatomical structures within the imaged volume in which there is no active uptake of radiotracer and, therefore, are likely to not be implicated in the LBP. Cervical facet joint, one of the potential sources of spinal and extremity pain, is susceptible to arthritic changes, degenerative process, inflammation, and injury and all of which will lead to painful event upon movement and restriction in range of neck motion. A definite diagnosis will help us to make sure the exact reason for the discomfort.
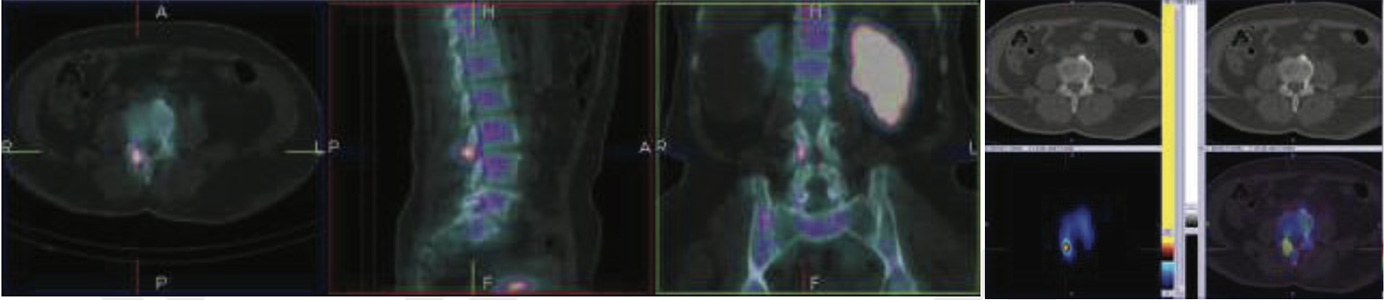
61 years old lady with 12 months history of non-localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral L5/S1 facet joints arthropathy (left>>right).

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
65 years old lady with 6 months history of non-localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral L5/S1 facet joints arthropathy (right>left).

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
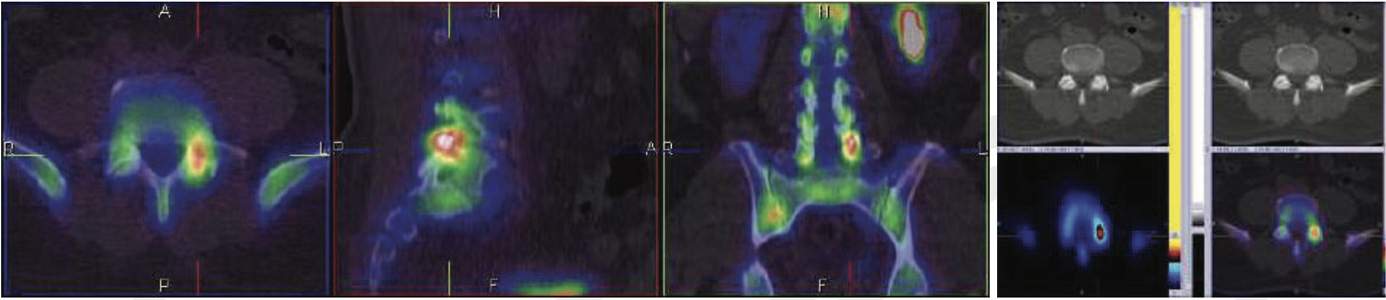
66-year-old gentleman with clinically generalized chronic neck pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized left C2/C3 & right C5/C6 facet joint arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF NECK REGION
62-year-old lady with clinically chronic neck pain. (mostly on left side) SPECT images, low dose CT and fused SPECT/CT bone images show localized left C3/C4 facet joint arthropathy.

55 years old lady with 9 months history of localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized left L5/S1 facet joints arthropathy.
99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
90 years old gentleman with 15 months history of non-localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized right L5/S1 & left L4/L5facet joints arthropathy (L5/S1 facet joint abnormality is more active than the L4/L5 facet joint abnormality).

66 years old gentleman with 24 months history of generalized back pain (more to in neck & lower back). SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral C4/C5 facet joints arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF NECK REGION

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION SPECT images, low dose CT and fused SPECT/CT bone images show localized left L4/l5 facet joints arthropathy.
74 years old gentleman with 8 months history low back pain SPECT images, low dose CT and fused SPECT/CT bone images show localized right L3/L4 facet joints arthropathy.
99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
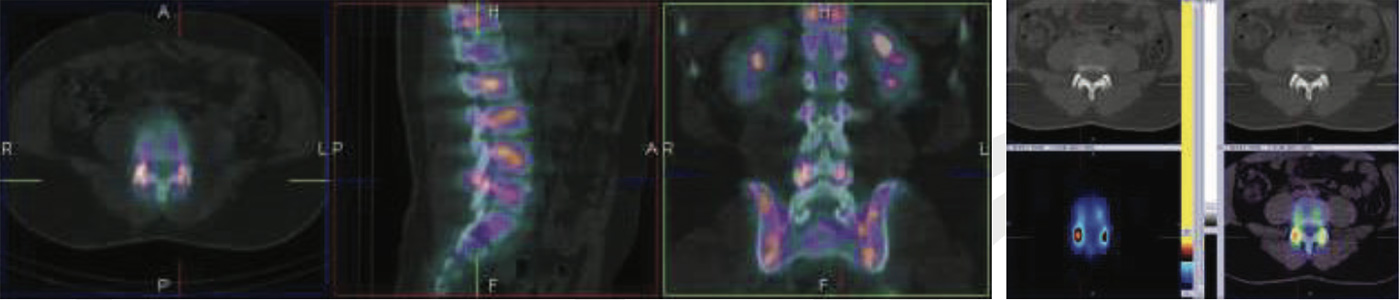
46 years old gentleman with 16 months history of localized low backpain. SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral L5/S1 facet joints arthropathy

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
59 years old lady with 8 months history of low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized right L4/L5 facet joints arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
59 years old lady with 5 months history of localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral L4/L5 facet joints arthropathy (right>left).
99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
57 years old lady with 18 months history of localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show localized bilateral L4/L5 facet joints arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
49 years old lady is a case of cancer breast (operated) with 7 months history of low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show Bilateral localized bilateral L5/S1 facet joints arthropathy (left>>right).

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
49 years old lady is a case of cancer breast (operated) with 7 months history of low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show Bilateral localized bilateral L5/S1 facet joints arthropathy (left>>right).

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
65 years old gentleman with 12 months history of right sided localized low back pain. SPECT images, low dose CT and fused SPECT/CT bone images show right localized L5/S1 facet joints arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
78 years old gentleman with few months’ history of left sided localized low back pain. Known case of ca prostate. SPECT images, low dose CT and fused SPECT/CT bone images show left localized L4/L5 facet joints arthropathy.

99mTc-MDP BONE SPECT CT FUSED IMAGES OF LUMBOSACRAL REGION
The fusion of anatomic and molecular images obtained with integrated SPECT/CT systems allows more accurate attenuation correction and precise anatomic localization of lesions with increased tracer uptake. SPECT/CT increases reporter confidence in the correct localization of uptake compared to simple planar or SPECT studies. SPECT/CT also enables the detection of tracer avid lesions. that are not appreciated by simple planar scintigraphy or SPECT performed without co-registered CT. When performed supplementary to conventional imaging techniques, the SPECT/CT images have an incremental diagnostic value that can influence clinical management by selecting only SPECT positive facet joint targets. Once the diagnostic information provided by the SPECT/CTs was available to the treating clinicians, patients proceeded to have either steroids injection, conservative or surgical interventions.
In the majority of patients studied, the SPECT/CT scan guided the referring clinicians in determining further clinical management, mainly by providing precise localization of SPECT positive fact joint arthropathy.