Thyroid scintigraphy holds a key place in the etiologic workup of neonatal hypothyroidism. Routine screening for this disorder in maternity hospitals in industrialized countries, for nearly 40 years, has permitted early treatment and thereby helped to prevent its physical and mental complications. Neonatal hypothyroidism affects approximately 1 in 3000 births. The most common causes are abnormal thyroid gland development and defective hormone synthesis by an eutopic thyroid gland. The incidence of the latter has risen in recent years, for reasons that remain unclear. Current guidelines recommend thyroid imaging by means of ultrasound and scintigraphy. Ultrasound should be done by a practitioner trained to examine the cervical region of newborns, as the thyroid is very small and must be distinguished from the particular aspect of the “thyroid empty lodge.” Ultrasound lacks sensitivity for detecting small ectopic glands but is the gold standard for measuring thyroid dimensions. Scintigraphy provides an etiologic diagnosis in most cases. The isotope used in this setting are technetium-99m. The latter isotope gives more contrast and allows the perchlorate discharge test to be performed to detect abnormal organification in the neonate with an eutopic thyroid. If scintigraphy cannot be performed during the neonatal period, a postponed procedure can be achieved after 3 years of age. Close cooperation between the nuclear medicine physician and the pediatric endocrinologist / Pediatricians is crucial for timely and optimized scintigraphy.
Dyshormonogenesis results from a deficiency or absence of one or more of the enzymes involved in thyroid hormone synthesis or secretion. Patients with peroxidase deficiency frequently have an enlarged gland (although it may be normal sized), an elevated TSH (due to decreased levels of circulating thyroid hormone), and a high uptake Tc-pertechnetate. Deficient peroxidase activity associated with a familial goitre and deafness or hearing loss is referred to as Pendred's syndrome.
This test is used to identify congenital or acquired organification defects which most commonly involves the enzyme iodide peroxidase.
In patients with defects in peroxidase activity (usually hypothyroid), trapped Tc-pertechnetate/radioiodine is rapidly discharged when sodium perchlorate (an inhibitor of thyroid iodide trapping) is administered.
Potassium perchlorate 109 mg/kg is then administered orally and a decrease in Tc-uptakes/RAIU greater than 10-15% following perchlorate administration is indicative of any organocation defect.
28-days old female, USG thyroid-Diffuse thyromegaly,
TSH 13.87, T4-10.9, TgAb and TPO antibodies were negative.
99mTc thyroid Scan- shows Tc uptakes 18% (0.4% - 3.0%), tracer distribution is patchy and relatively inhomogeneous but increased.
Post perchlorate images shows complete washout of the tracer from the thyroid gland, suggestive of Dyshormonogenesis / organification defect.
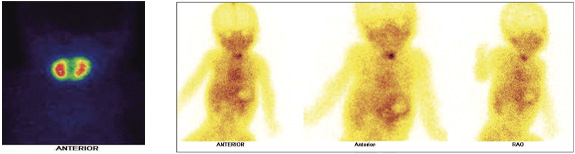
12 days old baby with TSH > 100, USG thyroid- Diffuse thyromegaly
99mTc thyroid Scan- shows enlarged thyroid gland with elevated uptakes. Tracer distribution is uniform and increased. It colud be due to a) Secondary to elevated maternal antibodies b) Disharmonogenesis.
3 days old baby diagnosed with congenital hypothyroidism. Mother has hypothyroidism and TSH receptor antibodies positive.
TSH 85.54 and free T$ 17.66 pmol/L, USG thyroid- normal in size, echogenicity and vascularity of the thyroid gland.
99mTc thyroid Scan- shows tracer asymmetrical and comparatively tracer uptakes in thyroid gland (left lobe functioning better than the right lobe), secondary to elevated maternal antibodies ( most likely).
24 days old baby diagnosed with congenital hypothyroidism.
TSH >100 (0.72- 11.0 miu/ml), FT4 3.0 (11.5-28.3 pmol/L, TgAb and TPO antibodies were negative. USG thyroid-Diffuse thyromegaly.
99mTc thyroid Scan- shows Tc uptakes 18.3% (0.4% - 3.0%) , enlarged thyroid gland, tracer distribution is patchy & asymmetrical but increased favoring Dyshormonogenesis /organification defect.
Newborn baby with features of hypothyroidism
TFT abnormal (high TSH).
USG thyroid- No appreciable thyroidal tissue.
99mTc thyroid Scan- shows no appreciable tracer uptakes in thyroid bed nor elsewhere suggestive of agenesis of thyroid gland.
24 days old baby diagnosed with congenital hypothyroidism.
TFT > 100abnormal.
USG thyroid- No appreciable thyroidal tissue.
99mTc thyroid Scan- shows no appreciable tracer uptakes in thyroid bed nor elsewhere suggestive of agenesis of thyroid gland.
Newly born baby diagnosed with congenital hypothyroidism.
TSH: 323, FT3: 2.5 (low), FT4: 0.65
99mTc thyroid Scan- shows small focal area of tracer uptakes in lingual region. No tracer uptakes seen in thyroidal bed favoring presence of ectopic functioning thyroid tissue in lingual region.
In Neonates with Congential Hypothyroidism 1) Isotope thyroid scan is a valuable imaging modality with low radiation burden 2) Isotope thyroid scan is not used to diagnose the condition but demonstrate the presence or absence of functioning thyroid tissue.
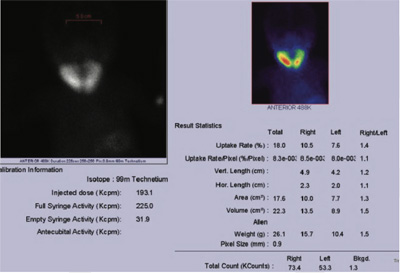
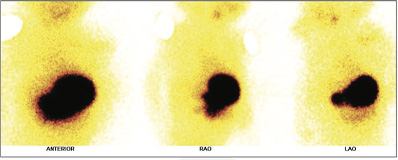
Figure 1: 99mTc thyroid scan with uptakes.
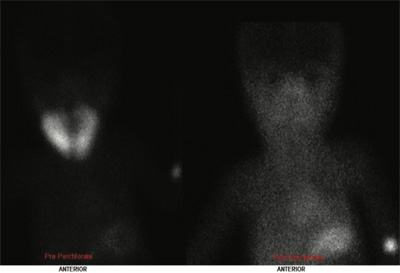
Figure 2: 99mTc thyroid scan a) thyroid images ( left) b) Post perchlorate washout thyroid images (right).
99mTc thyroid Scan- shows Tc uptakes 18%, tracer distribution is patchy and relatively inhomogeneous but increased.
Post perchlorate images shows complete washout of the tracer from the thyroid gland, suggestive of Dyshormonogenesis /organification defect.
99mTc thyroid Scan- shows enlarged thyroid gland with elevated uptakes. Tracer distribution is uniform and increased.
It colud be due to a) Secondary to elevated maternal antibodies b) Disharmonogenesis.
99mTc thyroid Scan- shows tracer asymmetrical and comparatively tracer uptakes in thyroid gland (left lobe functioning better than the right lobe), secondary to elevated maternal antibodies ( most likely).
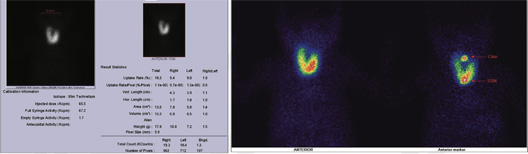
99mTc thyroid Scan- shows Tc uptakes 18.3% (0.4% - 3.0%) , enlarged thyroid gland, tracer distribution is patchy & asymmetrical but increased favoring Dyshormonogenesis /organification defect.

99mTc thyroid Scan- shows no appreciable tracer uptakes in thyroid bed nor elsewhere suggestive of agenesis of thyroid gland.
99mTc thyroid Scan- shows no appreciable tracer uptakes in thyroid bed nor elsewhere suggestive of agenesis of thyroid gland.
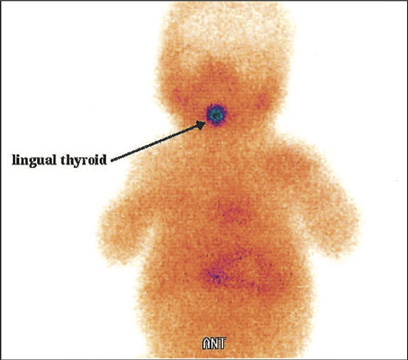
99mTc thyroid Scan- shows small focal area of tracer uptakes in lingual region.
No tracer uptakes seen in thyroidal bed favoring presence of ectopic functioning thyroid tissue in lingual region.